For over 50 years, Millar's high-fidelity, integrated pressure sensing devices have helped record measurements of cardiovascular function and monitored clinical conditions like pulmonary hypertension, congenital heart disease, mechanical circulatory support, peripheral vascular, left ventricle pressure, valvular disorders, and more. These cardiovascular pressure measurements provide in-depth data to assess heart failure conditions. Millar's absolute and vented pressure sensor designs fit within a 1F (.013") encasement and measure pressures from -760 to 4000 mmHg (-101 to 533 kPa). Our integrated high-fidelity sensors can reduce sources of error typical of fluid-filled right heart pressure measurements and provide feedback data in various circulatory assist devices.
Since 1969, Millar’s products have played a significant role in cardiovascular medical device innovation, providing deeper insights into cardiovascular function and helping guide diagnostic decisions when precise measurements count. Learn more in the application examples below:
Left Ventricular Pressure (LVP)
When evaluating pericarditis, fluid-filled transducers are generally used to measure left ventricular pressure and right ventricular pressure for comparison of LV and RV waveform areas during inspiration and expiration. In patients with constrictive pericarditis, these changes are discordant. The patient’s LV systolic pressure increases during expiration do not correlate with expected RV systolic pressure increases. The patient’s LV systolic pressure decreases during inspiration show increases in RV systolic pressures.
Millar’s Mikro-Cath™ Pressure Catheter provides a direct high-fidelity measure of right and left ventricular blood pressure, resulting in cleaner waveform tracings and easier identification of discordant systolic and diastolic values for comparison purposes.
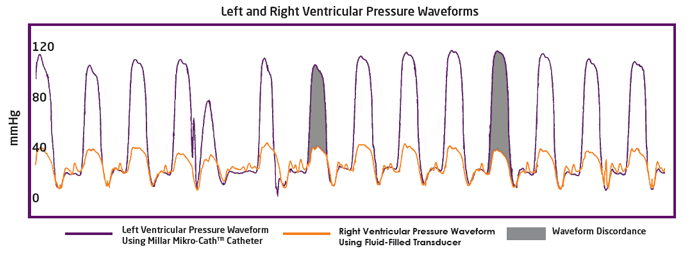
In this example, a patient suspected of having constrictive pericarditis was catheterized with a Mikro-Cath™ for left ventricular pressure measurement and a fluid-filled transducer for right ventricular pressure measurement. The data collected from the Mikro-Cath™ pressure catheter was able to provide precise insight as to the patient's cardiovascular condition and aid the clinician in identifying the discordance in the LV and RV systolic pressures.
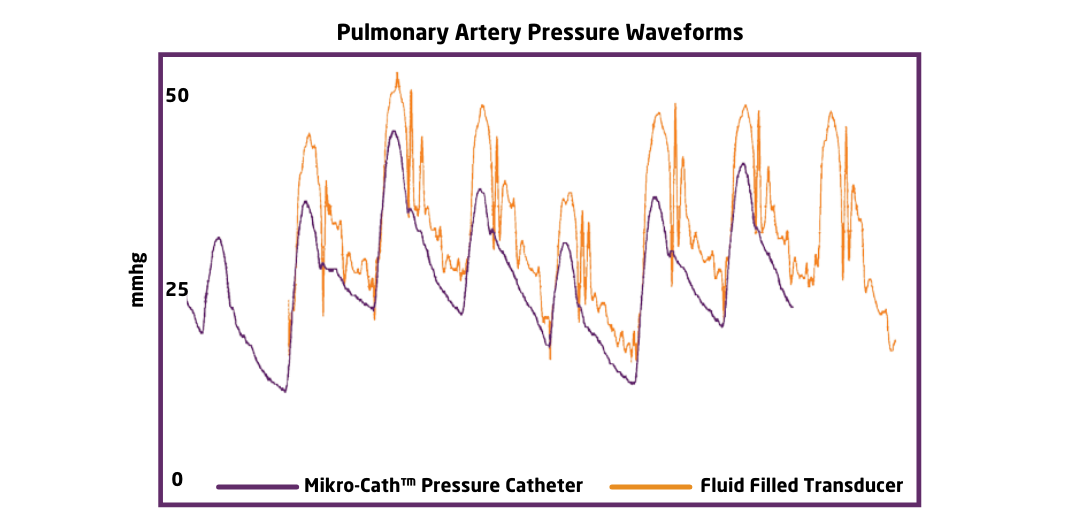
Pulmonary Artery Pressure (PAP)
Pulmonary Artery Pressure (PAP) is one of the most commonly measured parameters during a cardiac catheterization case. Mean PAP, systolic PAP and diastolic PAP are often derived by visually marking the waveform output by a fluid-filled transducer. This waveform is influenced by a number of factors, including patient position, transducer level, air bubbles, open connections and catheter tubing length, all of which can introduce error into the measurement. The result is a potential for over-estimation or under-estimation of the systolic and diastolic values.
The Millar Mikro-Cath™ diagnostic pressure catheter can be introduced into the pulmonary artery via a 6F or larger multi-purpose catheter to deliver a more accurate and reproducible PAP waveform, independent of the factors that impact fluid-filled readings. The result is a simplification in both the recording and reading of PAP derived parameters.
The waveform diagram below highlights the differences between the Mikro-Cath™ and fluid-filled pressure transducers. The recordings were made in the same patient several minutes apart and have been overlaid for comparison.
Cardiac Resynchronization Therapy (CRT)
Cardiac Resynchronization Therapy (CRT) is an effective treatment performed in systolic heart failure patients with a wide QRS complex. The presence of a wide QRS complex indicates a block in the right or left bundle branches or non-specific delay. This block or delay causes ventricular depolarization to travel through the myocardium instead of the His-Purkinje system. CRT uses electrical leads to optimize ventricular contractions by bypassing the heart’s depolarization system. These leads then control ventricular depolarization to narrow the QRS width and improve the heart’s efficiency. However, factors such as the heart tissue’s response to stimulation, the absence of desynchrony, or the inability to achieve optimal lead placement contribute to CRT treatment failure in 30% of patients.
Several studies have shown success with CRT implantation by using Millar solid-state Mikro-Cath™ pressure catheters. Using a Millar Mikro-Cath™ in conjunction with imaging or pacing technologies, such as the Schwarzer Cardiotek EP-Tracer recording system, clinicians can optimize lead placement in real-time by assessing parameters such as left ventricular (LV) volume, ejection fraction, QRS width, LV pressure, and dP/dtmax. When compared to fluid-filled catheters, the Mikro-Cath provides real-time, accurate blood pressure data, measuring blood pressure at the source and providing a true representation of the blood pressure waveform. This eliminates many of the common shortfalls of fluid-filled catheters, including signal variances from patient height or position changes.
As the gold standard of pressure measurement, and with a continued focus on innovation, Millar plans to stay ahead of the curve by continually pushing the limits of medical device understanding across the cardiovascular market and beyond - helping guide diagnostic decisions when precise measurements count.